CMS 149v12: Dementia: Cognitive Assessment
| Measure: Percentage of patients, regardless of age, with a diagnosis of dementia for whom an assessment of cognition is performed and the results reviewed at least once within a 12-month period | ||
| Measure Type | High Priority Measure | Scoring |
| Process | Yes | A higher percentage indicates better quality |
| Denominator | All patients, regardless of age, with a diagnosis of dementia |
| Numerator | Patients for whom an assessment of cognition is performed and the results reviewed at least once within a 12-month period |
| Denominator Exceptions | Documentation of patient reason(s) for not assessing cognition |
| Denominator Exclusions | None |
Patients who meet the following criteria will be included in the denominator:
-
Have an eligible encounter with an active diagnosis of dementia during the Measurement Period finalized by the EC
AND
- Have at least one eligible qualifying encounter during the Measurement Period finalized by the EC
CPT: 90791, 90792, 90832, 90834, 90837, 96116, 97165, 97166, 97167, 97168, 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99241, 99242, 99243, 99244, 99245, 99304, 99305, 99306, 99307, 99308, 99309, 99310, 99315, 99316, 99318, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350
Diagnoses are documented in the Assessment tab of an encounter. The eligible diagnosis codes for dementia are:
ICD-10: A52.17, F01.50, F02.80, F03.90, F05, F06.8, G30.0, G30.1, G30.8, G30.9, G31.01, G31.09, G31.83
CPT: 90791, 90792, 90832, 90834, 90837, 96116, 97165, 97166, 97167, 97168, 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99241, 99242, 99243, 99244, 99245, 99304, 99305, 99306, 99307, 99308, 99309, 99310, 99315, 99316, 99318, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 99441, 99442, 99443, 99421, 99422, 99423, 99024, 99251, 99252, 99253, 99254, 99255
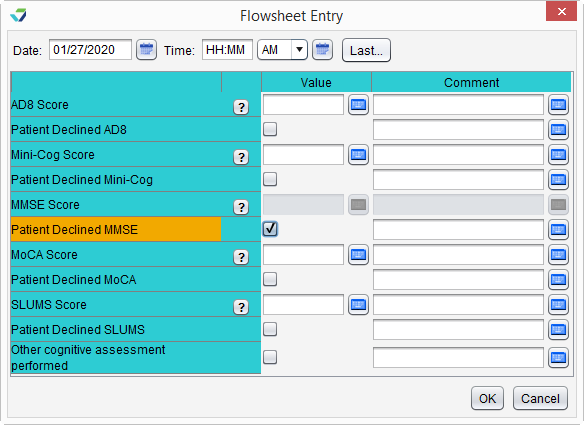
A patient will be counted as an exception for this measure if there is a documented patient reason for not performing a cognitive assessment.
- Go to Encounter > Flowsheets/Labs > Standard or Chart > Flowsheets/Labs > Standard
- Click Add New Flowsheet
- Select the Cognitive Assessment flowsheet and click Add
- Click Add Column
- Select the 'Patient declined...' checkbox for the AD8, Mini-Cog, MMSE, MoCA, or SLUMS assessment
- Click OK to save
- Go to Encounter > Orders/Procedure > Orders/Referrals
-
Click Add to add one of the following eligible codes:
SNOMED CT: 113024001, 4719001
- Order Status must be Not Performed
- Not Performed Reason must be Refusal of treatment by patient
- Click Add to save
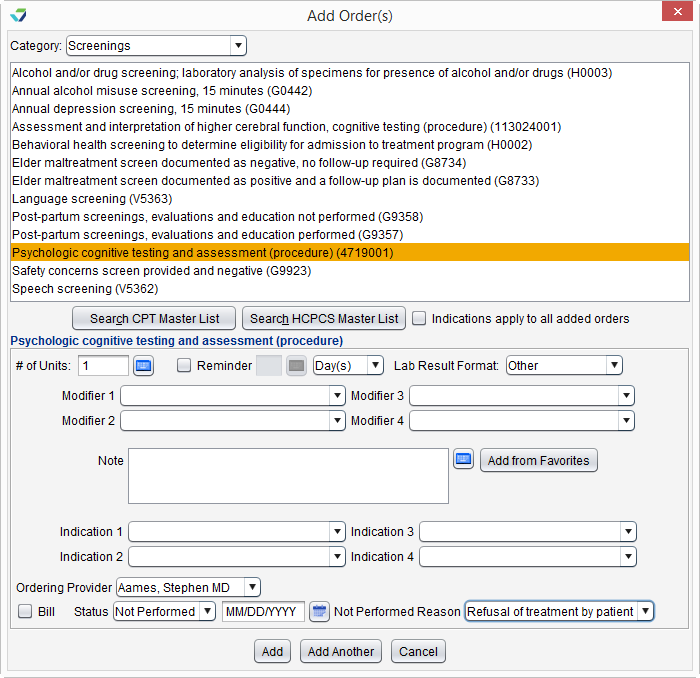
SNOMED CT codes must be added as a Favorite in Preferences > Form Data > Orders to be accessible from the Orders/Referrals tab
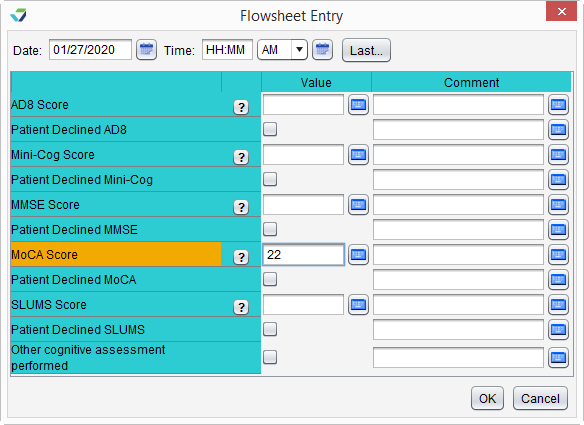
A patient will be counted in the numerator if they received a cognitive assessment using a standardized screening on the day of their eligible dementia encounter or in the 12 months before their eligible dementia encounter.
To document a screening using the Cognitive Assessment flowsheet:
- Go to Encounter > Flowsheets/Labs > Standard or Chart > Flowsheets/Labs > Standard
- Click Add New Flowsheet
- Select the Cognitive Assessment flowsheet and click Add
- Click Add Column
-
Populate the patient's score for the AD8, Mini-Cog, MMSE, MoCA, or SLUMS assessment
or
Select the Other cognitive assessment performed checkbox
- Click OK to save
If Other cognitive assessment performed is selected, the name of the screening tool should be documented in the encounter in which it was performed
Return to 2024 eCQMs
Didn't find the answer you were looking for?
Contact Sevocity Support 24/7 at 877‑777‑2298 or support@sevocity.com