CMS 124v12: Cervical Cancer Screening
|
Measure: Percentage of women 21-64 years of age who were screened for cervical cancer using either of the following criteria:
|
||
| Measure Type | High Priority Measure | Scoring |
| Process | No | A higher percentage indicates better quality |
| Denominator | Women 24-64 years of age by the end of the measurement period with a visit during the measurement period |
| Numerator |
Women with one or more screenings for cervical cancer. Appropriate screenings are defined by any one of the following criteria:
|
| Denominator Exceptions | None |
| Denominator Exclusions |
|
This eCQM requires a lab interface to be met. Customers interested in a lab interface should contact Sevocity Support to begin the process of a new interface setup. Interface setup requirements and fees vary per request.
Patients who meet the following criteria will be included in the denominator:
-
Have a birth sex of female
AND
-
Age is 24 years to 64 years at the end of the Measurement Period
AND
- Have at least one eligible encounter during the Measurement Period finalized by the EC
CPT: 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99395, 99396, 99397, 99385, 99386, 99387, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 98969, 98970, 98971, 98972, 99421, 99422, 99423, 99458, 98966, 98967, 98968, 99441, 99442, 99443, 98980, 98981, 99444, 99457
HCPCS: G0071, G2010, G2012, G2061, G2062, G2063, G2250, G2251, G2252
A patient will be excluded from this measure if they meet any of the following conditions:
- Had a hysterectomy with no residual cervix performed any time before the end of the Measurement Period
- Has an active or resolved diagnosis of a hysterectomy with no residual cervix
- Has a documented medical history of congenital absence of the cervix
- Has an active diagnosis of congenital or acquired absence of the cervix
- Is in hospice care for any part of the Measurement Period
- Is receiving palliative for any part of the Measurement Period
To document the performance of a hysterectomy, go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
CPT: 57530, 57531, 57540, 57545, 57550, 57555, 57556, 58150, 58152, 58200, 58210, 58240, 58260, 58262, 58263, 58267, 58270, 58275, 58280, 58285, 58290, 58291, 58292, 58293, 58294, 58548, 58550, 58552, 58553, 58554, 58570, 58571, 58572, 58573, 58575, 58951, 58953, 58954, 58956, 59135
Order Status must be marked as Complete.
Diagnoses are documented in the Assessment tab of an encounter. The eligible diagnosis code for hysterectomy with no residual cervix is:
ICD-9: 618.5
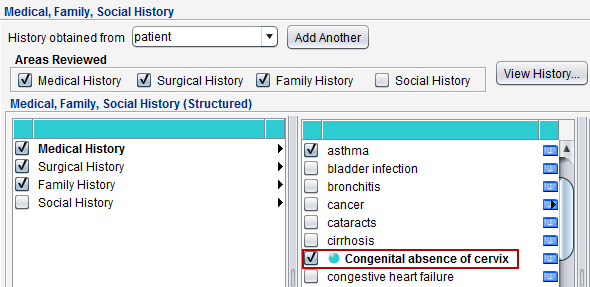
- Go to Encounter > Past History > Structured > Medical History
- Select the hardcoded Congenital absence of cervix node
Diagnoses are documented in the Assessment tab of an encounter. The eligible diagnosis codes for congenital or acquired absence of cervix are:
ICD-10: Q51.5, Z90.710, Z90.712
ICD-9: 618.5, 752.43, V88.01, V88.03
To document hospice care ambulatory services, go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
CPT: 99377, 99378
HCPCS: G0182
Order Status must be marked as Pending or Complete.
To document hospice care encounter services, go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
HCPCS: G9996, G9473, G9474, G9475, G9476, G9477, G9478, G9479, Q5003, Q5004, Q5005, Q5006, Q5007, Q5008, Q5010, S9126, T2042, T2043, T2044, T2045, T2046
Order Status must be marked as Complete.
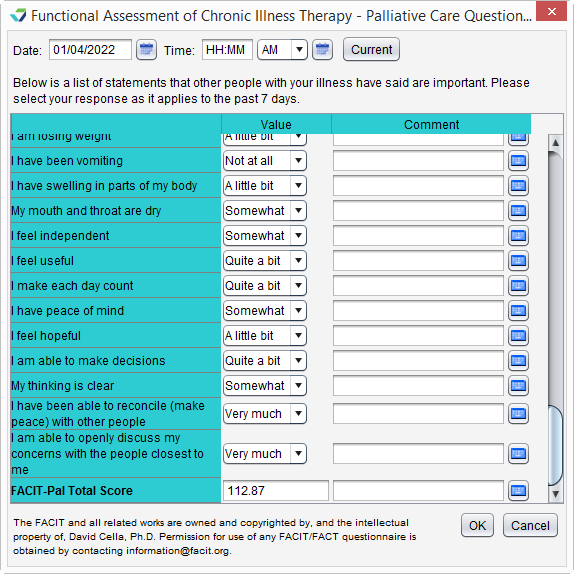
Palliative care services can be documented using the FACIT-Pal Questionnaire flowsheet, as an order, or as a diagnosis.
-
Go to Encounter > Flowsheets/Labs > Standard or Chart > Flowsheets/Labs > Standard
-
Click Add New Flowsheet
-
Select the FACIT-Pal Questionnaire flowsheet and click Add
-
Click Add Column
-
Populate the patient's responses to the questions as appropriate
-
Click OK to save
Go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
HCPCS: G9054, M1017
Order Status must be marked as Complete.
Diagnoses are documented in the Assessment tab of an encounter. The eligible diagnosis code for palliative care is:
ICD-10: Z51.5
A patient will be counted in the numerator if they received at least one screening for cervical cancer. Appropriate screenings and time frames for cervical cancer are defined as follows:
-
At least one Pap test performed during the Measurement Period or in the 2 years prior
-
The patient must be 21 years or older at the time of the test
OR
-
- For patients aged ≥ 30 years, one HPV test performed during the Measurement Period or in the 4 years prior
- The patient must be 30 years or older at the time of the test
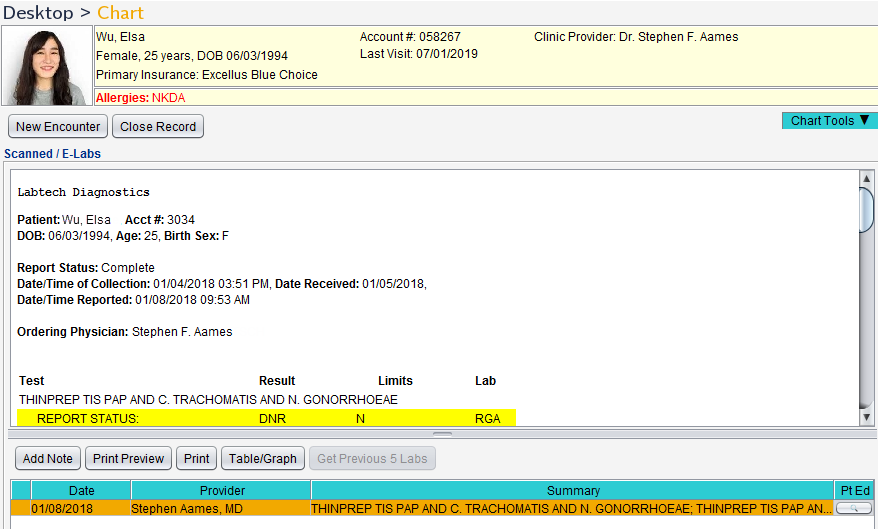
To document that a Pap test or an HPV test was performed, an e-Lab result for the test must be stored to the patient chart.
- From the Clinic Inbox, select the lab result to be stored and click View
- If the lab result is systematically matched to a patient, the Patient section will be populated in the lab result display
- If the lab result is not matched or the matched patient needs to be changed, the user will need to search for the patient
- Optional: click Select to search for and select a patient
- Select the I have verified the following lab results belong to the above patient checkbox
- Click Sign/Route
- Select the Sign checkbox and click OK
Stored e-Lab results can be viewed in the Flowsheets/Labs > Scanned/E-Labs tab of the patient chart.
Return to 2024 eCQMs
Didn't find the answer you were looking for?
Contact Sevocity Support 24/7 at 877‑777‑2298 or support@sevocity.com