CMS 130v10: Colorectal Cancer Screening
| Measure: Percentage of adults 50-75 years of age who had appropriate screening for colorectal cancer | ||
| Measure Type | High Priority Measure | Scoring |
| Process | No | A higher percentage indicates better quality |
| Denominator | Patients 50-75 years of age with a visit during the measurement period |
| Numerator | Patients with one or more screenings for colorectal cancer. Appropriate screenings are defined by any one of the following criteria:
|
| Denominator Exceptions | None |
| Denominator Exclusions |
|
A lab interface can be used to meet this eCQM but is not required. Customers interested in a lab interface should contact Sevocity Support to begin the process of a new interface setup. Interface setup requirements and fees vary per request.
Patients who meet the following criteria will be included in the denominator:
Age is ≥ 50 years and < 75 years at the beginning of the Measurement Period
AND
- Have at least one eligible encounter during the Measurement Period finalized by the EC
CPT: 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99395, 99396, 99397, 99385, 99386, 99387, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 98969, 98970, 98971, 98972, 99421, 99422, 99423, 99458, 98966, 98967, 98968, 99441, 99442, 99443
HCPCS: G0438, G0439, G0071, G2010, G2012, G2061, G2062, G2063
A patient will be excluded from the measure if they meet any of the following conditions:
- Has an active diagnosis of colorectal cancer during the Measurement Period
- Had a total colectomy
- Is in hospice care for any part of the Measurement Period
- Is receiving palliative care during the Measurement Period
- Age is ≥ 65 at the start of the Measurement Period and has spent more than 90 consecutive days during the Measurement Period living in long term care
- Age is ≥ 65 at the start of the Measurement Period and has evidence of frailty and advanced illness
Diagnoses are documented in the Assessment tab of an encounter. A comprehensive list of eligible diagnosis codes for malignant neoplasm of the colon can be located here.
To document a total colectomy procedure, go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
CPT: 44150, 44151, 44152, 44153, 44155, 44156, 44157, 44158, 44210, 44211, 44212
Order Status must be marked as Complete.
To document hospice care services as a procedure, go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
SNOMED CT: 385763009, 385765002
Order Status must be marked as Pending or Complete.
SNOMED CT codes must be added as a Favorite in Preferences > Form Data > Orders to be accessible from the Orders/Referrals tab.
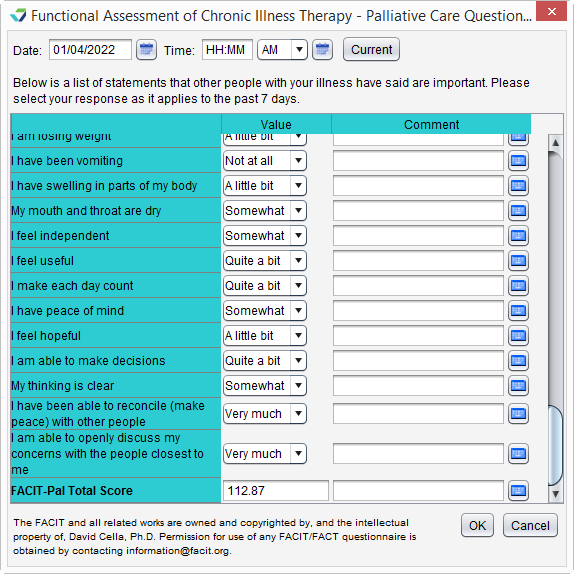
Palliative care services can be documented using the FACIT-Pal Questionnaire flowsheet or in the Orders/Procedure tab.
Go to Encounter > Flowsheets/Labs > Standard Flowsheets
Click Add New Flowsheet
Select the FACIT-Pal Questionnaire flowsheet and click Add
Click Add Column
Populate the patient's responses to the questions as appropriate
Click OK to save
Go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
HCPCS: G9054, M1017
Order Status must be marked as Complete.
To document a stay in long term care:
- Go to Chart > Admissions and click Add
- Select a Place of Service
- Optional: select a Facility
- Populate the Admit Date
- Optional: populate the Discharge Date
- Click OK
If the admissions event does not have a Discharge Date when the eCQM report is generated, the length of stay will be calculated with a discharge date of the Reporting Period end date or the Measurement Period end date, whichever occurs first.
A patient has evidence of frailty if they meet any of the following criteria:
- Has an active diagnosis of Frailty during the Measurement Period
- Has an active diagnosis of Frailty Symptom during the Measurement Period
- Is using a frailty device during the Measurement Period
- Has a frailty encounter during the Measurement Period
"Frailty" refers to a range of conditions that includes falls and problems affecting mobility.
Diagnoses are documented in the Assessment tab of an encounter. A comprehensive list of eligible diagnosis codes for frailty can be located here.
Diagnoses are documented in the Assessment tab of an encounter. The eligible diagnosis codes for frailty symptoms are:
ICD-10: R26.0, R26.1, R26.2, R26.89, R26.9, R41.81, R53.1, R53.81, R53.83, R54, R62.7, R63.4, R63.6, R64
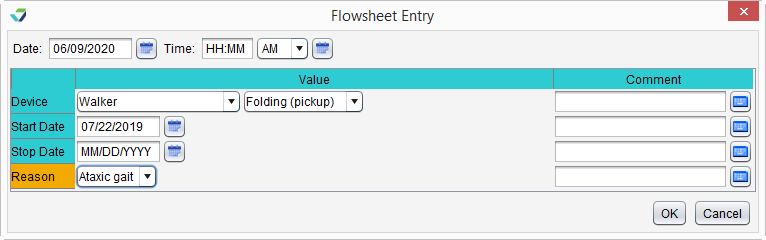
To document the patient's use of a frailty device:
- Go to Encounter > Flowsheets/Labs > Standard Flowsheets
- Click Add New Flowsheet
- Select the Frailty Device flowsheet and click Add
- Click Add Column
- Select a Device and the type (Value) of device
- Populate a usage Start Date for the device
- Optional: populate a usage Stop Date for the device
- The Stop Date cannot occur prior to the start of the Measurement Period
- Optional: populate a Reason for use of the device
- Click OK to save
CPT: 99504, 99509
HCPCS: G0162, G0299, G0300, G0493, G0494, S0271, S0311, S9123, S9124, T1000, T1001, T1002, T1003, T1004, T1005, T1019, T1020, T1021, T1022, T1030, T1031
A patient has evidence of advanced illness if they meet any of the following criteria:
- Had an inpatient encounter with an active diagnosis of Advanced Illness during the Measurement Period or in the year prior
- Had 2 or more outpatient encounters with an active diagnosis of Advanced Illness during the Measurement Period or in the year prior
- Encounters must have different dates of service
- Diagnosis must be active during all eligible encounters
- Was prescribed medication for dementia during the Measurement Period or in the year prior
"Advanced illness" refers to a wide range of conditions and includes diseases such as Alzheimer's disease, cancer, and heart failure.
Diagnoses are documented in the Assessment tab of an encounter. A comprehensive list of eligible diagnosis codes for advanced illness can be located here.
CPT: 99221, 99222, 99223, 99231, 99232, 99233, 99238, 99239, 99251, 99252, 99253, 99254, 99255, 99291
CPT: 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, 99215, 99241, 99242, 99243, 99244, 99245, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 99381, 99382, 99383, 99384, 99385, 99386, 99387, 99391, 99392, 99393, 99394, 99395, 99396, 99397, 99401, 99402, 99403, 99404, 99411, 99412, 99429, 99455, 99456, 99483, 99217, 99218, 99219, 99220, 99281, 99282, 99283, 99284, 99285, 99304, 99305, 99306, 99307, 99308, 99309, 99310, 99315, 99316, 99318, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337
HCPCS: G0402, G0438, G0439, G0463, T1015
To prescribe a medication, go to Encounter > Medications > Manage/Prescribe Meds > New Prescription. A comprehensive list of eligible dementia medications can be located here.
A patient will be counted in the numerator if they received at least one of the following colon cancer screenings:
- FOBT during the Measurement Period
- Flexible sigmoidoscopy during the Measurement Period or in the 4 years prior
- Colonoscopy during the Measurement Period or in the 9 years prior
- FIT-DNA test during the Measurement Period or in the 2 years prior
- CT Colonography during the Measurement Period or in the 4 years prior
To document a colonoscopy or flexible sigmoidoscopy procedure, go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below. Order Status must be marked as Complete.
Colonoscopy
CPT: 44388, 44389, 44390, 44391, 44392, 44393, 44394, 44397, 44401, 44402, 44403, 44404, 44405, 44406, 44407, 44408, 45355, 45378, 45379, 45380, 45381, 45382, 45383, 45384, 45385, 45386, 45387, 45388, 45389, 45390, 45391, 45392, 45393, 45398
HCPCS: G0105, G0121
Flexible Sigmoidoscopy
CPT: 44397, 45330, 45331, 45332, 45333, 45334, 45335, 45337, 45338, 45339, 45340, 45341, 45342, 45345, 45346, 45347, 45349, 45350
HCPCS: G0104
To document that a CT Colonography, FOBT, or FIT-DNA test was performed, an e-Lab result for the test must be stored to the patient chart.
- From the Clinic Inbox, select the lab result to be stored and click View
- Click Select to search for and select a patient
- Verify patient displayed matches the lab result and select the I have verified the following lab results belong to the above patient checkbox
- Click Sign/Route
- Select the Sign checkbox and click OK
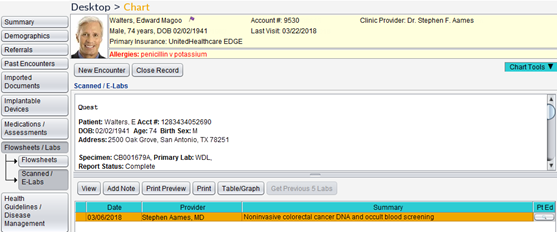
Stored e-Lab results can be viewed in the Flowsheets/Labs > Scanned/E-Labs tab of the patient chart.
Return to 2022 eCQMs
Didn't find the answer you were looking for?
Contact Sevocity Support 24/7 at 877‑777‑2298 or support@sevocity.com