CMS 125v10: Breast Cancer Screening
| Measure: Percentage of women 50-74 years of age who had a mammogram to screen for breast cancer in the 27 months prior to the end of the Measurement Period | ||
| Measure Type | High Priority Measure | Scoring |
| Process | No | A higher percentage indicates better quality |
| Denominator | Women 51-74 years of age with a visit during the measurement period |
| Numerator | Women with one or more mammograms during the 27 months prior to the end of the measurement period |
| Denominator Exceptions | None |
| Denominator Exclusions |
|
A lab interface can be used to meet this eCQM but is not required. Customers interested in a lab interface should contact Sevocity Support to begin the process of a new interface setup. Interface setup requirements and fees vary per request.
Patients who meet the following criteria will be included in the denominator:
Have a birth sex of female
AND
Age is ≥ 51 years and < 74 years at the beginning of the Measurement Period
AND
- Have at least one eligible encounter during the Measurement Period finalized by the EC
CPT: 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99395, 99396, 99397, 99385, 99386, 99387, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 98969, 98970, 98971, 98972, 99421, 99422, 99423, 99458, 98966, 98967, 98968, 99441, 99442, 99443,
HCPCS: G0438, G0439, G0071, G2010, G2012, G2061, G2062, G2063
A patient will be excluded from the measure if they meet any of the following conditions:
- Has an active or resolved diagnosis for a bilateral mastectomy or two unilateral mastectomies
- Has a documented medical history of a bilateral mastectomy or two unilateral mastectomies
- Is in hospice care for any part of the Measurement Period
- Is receiving palliative care during the Measurement Period
- Age is ≥ 65 at the start of the Measurement Period and has spent more than 90 consecutive days during the Measurement Period living in long term care
- Age is ≥ 65 at the start of the Measurement Period and has evidence of frailty and advanced illness
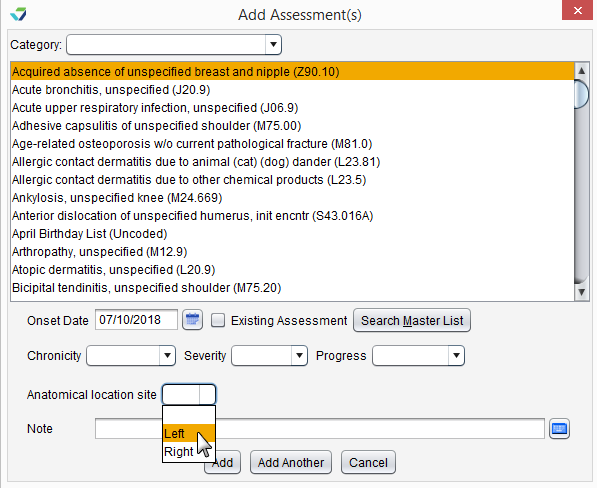
Diagnoses are documented in the Assessment tab of an encounter. The eligible diagnosis codes for this exclusion are:
Bilateral Mastectomy
ICD-10: Z90.13
Unilateral Mastectomy
ICD-10: Z90.10, Z90.11, Z90.12
ICD-9: V45.71
If documenting two unilateral mastectomies using a diagnosis code with unspecified laterality, the Anatomical Location Site for Left and Right must be specified when adding each diagnosis code.
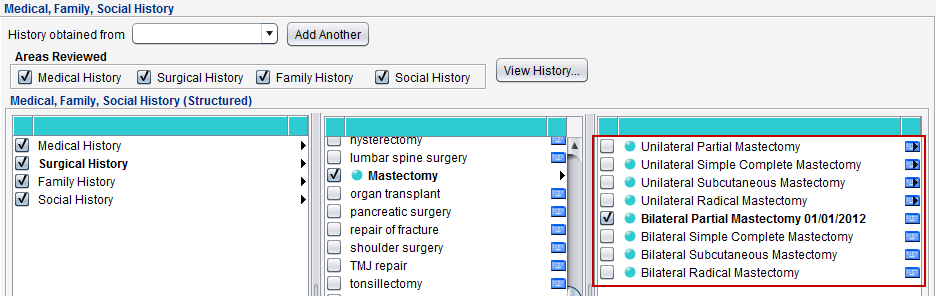
To document a bilateral or two unilateral mastectomies in the patient history:
- Go to Encounter > Past History > Structured > Surgical History
- Select the hardcoded Mastectomy node
- Select the appropriate bilateral or unilateral mastectomy type for the patient
- If selecting a unilateral mastectomy type, both Right Breast and Left Breast must be selected
- Populate the Date of Surgery for the mastectomy
- Click OK to save
To document hospice care services as a procedure, go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
SNOMED CT: 385763009, 385765002
Order Status must be marked as Pending or Complete.
SNOMED CT codes must be added as a Favorite in Preferences > Form Data > Orders to be accessible from the Orders/Referrals tab.
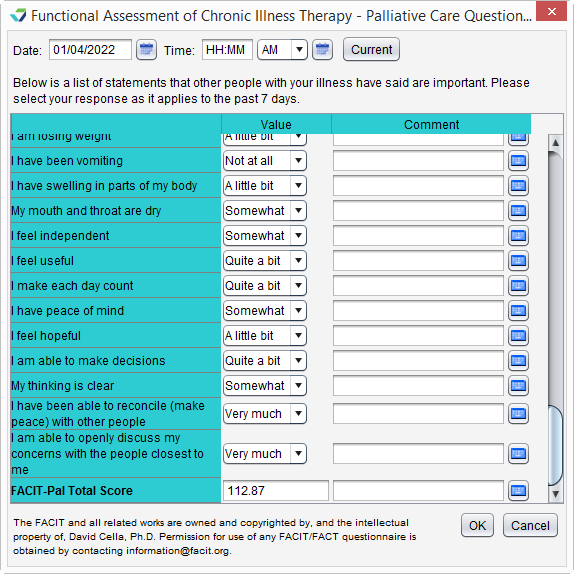
Palliative care services can be documented using the FACIT-Pal Questionnaire flowsheet or in the Orders/Procedure tab.
Go to Encounter > Flowsheets/Labs > Standard Flowsheets
Click Add New Flowsheet
Select the FACIT-Pal Questionnaire flowsheet and click Add
Click Add Column
Populate the patient's responses to the questions as appropriate
Click OK to save
Go to Encounter > Orders/Procedure > Orders/Referrals and click Add to add one of the eligible codes listed below:
HCPCS: G9054, M1017
Order Status must be marked as Complete.
To document a stay in long term care:
- Go to Chart > Admissions and click Add
- Select a Place of Service
- Optional: select a Facility
- Populate the Admit Date
- Optional: populate the Discharge Date
- Click OK
If the admissions event does not have a Discharge Date when the eCQM report is generated, the length of stay will be calculated with a discharge date of the Reporting Period end date or the Measurement Period end date, whichever occurs first.
A patient has evidence of frailty if they meet any of the following criteria:
- Has an active diagnosis of Frailty during the Measurement Period
- Has an active diagnosis of Frailty Symptom during the Measurement Period
- Is using a frailty device during the Measurement Period
- Has a frailty encounter during the Measurement Period
"Frailty" refers to a range of conditions that includes falls and problems affecting mobility.
Diagnoses are documented in the Assessment tab of an encounter. A comprehensive list of eligible diagnosis codes for frailty can be located here.
Diagnoses are documented in the Assessment tab of an encounter. The eligible diagnosis codes for frailty symptoms are:
ICD-10: R26.0, R26.1, R26.2, R26.89, R26.9, R41.81, R53.1, R53.81, R53.83, R54, R62.7, R63.4, R63.6, R64
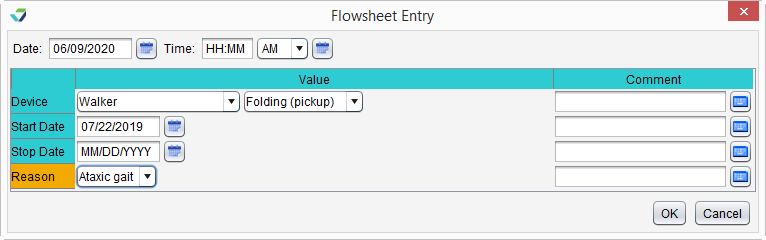
To document the patient's use of a frailty device:
- Go to Encounter > Flowsheets/Labs > Standard Flowsheets
- Click Add New Flowsheet
- Select the Frailty Device flowsheet and click Add
- Click Add Column
- Select a Device and the type (Value) of device
- Populate a usage Start Date for the device
- Optional: populate a usage Stop Date for the device
- The Stop Date cannot occur prior to the start of the Measurement Period
- Optional: populate a Reason for use of the device
- Click OK to save
CPT: 99504, 99509
HCPCS: G0162, G0299, G0300, G0493, G0494, S0271, S0311, S9123, S9124, T1000, T1001, T1002, T1003, T1004, T1005, T1019, T1020, T1021, T1022, T1030, T1031
A patient has evidence of advanced illness if they meet any of the following criteria:
- Had an inpatient encounter with an active diagnosis of Advanced Illness during the Measurement Period or in the year prior
- Had 2 or more outpatient encounters with an active diagnosis of Advanced Illness during the Measurement Period or in the year prior
- Encounters must have different dates of service
- Diagnosis must be active during all eligible encounters
- Was prescribed medication for dementia during the Measurement Period or in the year prior
"Advanced illness" refers to a wide range of conditions and includes diseases such as Alzheimer's disease, cancer, and heart failure.
Diagnoses are documented in the Assessment tab of an encounter. A comprehensive list of eligible diagnosis codes for advanced illness can be located here.
CPT: 99221, 99222, 99223, 99231, 99232, 99233, 99238, 99239, 99251, 99252, 99253, 99254, 99255, 99291
CPT: 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, 99215, 99241, 99242, 99243, 99244, 99245, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 99381, 99382, 99383, 99384, 99385, 99386, 99387, 99391, 99392, 99393, 99394, 99395, 99396, 99397, 99401, 99402, 99403, 99404, 99411, 99412, 99429, 99455, 99456, 99483, 99217, 99218, 99219, 99220, 99281, 99282, 99283, 99284, 99285, 99304, 99305, 99306, 99307, 99308, 99309, 99310, 99315, 99316, 99318, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337
HCPCS: G0402, G0438, G0439, G0463, T1015
To prescribe a medication, go to Encounter > Medications > Manage/Prescribe Meds > New Prescription. A comprehensive list of eligible dementia medications can be located here.
A patient will be counted in the numerator if they received a mammogram during the Measurement Period or in the 15 months before the start of the Measurement Period.
A mammogram can be documented as an e-lab result or from the Breast Cancer Screening flowsheet.
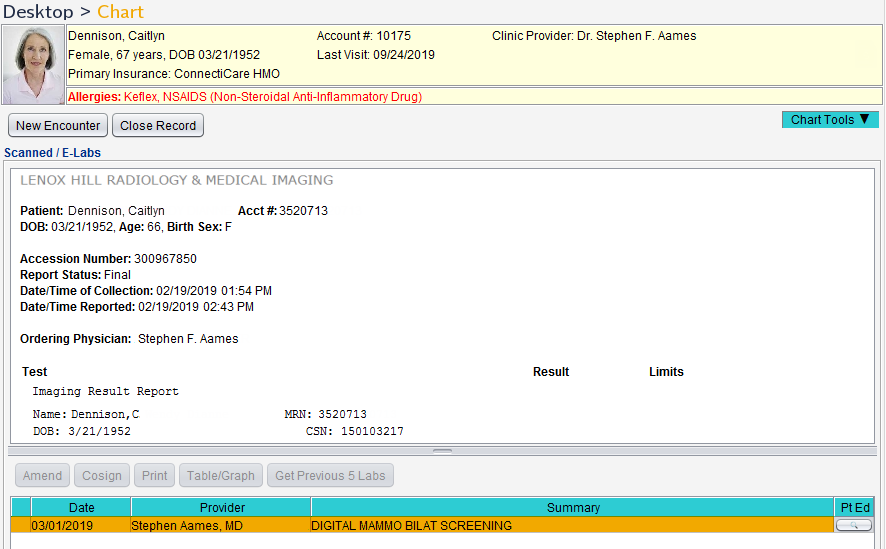
To document that a mammogram was performed, an e-Lab result for the test must be stored to the patient chart.
- From the Clinic Inbox, select the lab result to be stored and click View
- Click Select to search for and select a patient
- Verify patient displayed matches the lab result and select the I have verified the following lab results belong to the above patient checkbox
- Click Sign/Route
- Select the Sign checkbox and click OK
Stored e-Lab results can be viewed in the Flowsheets/Labs > Scanned/E-Labs tab of the patient chart.
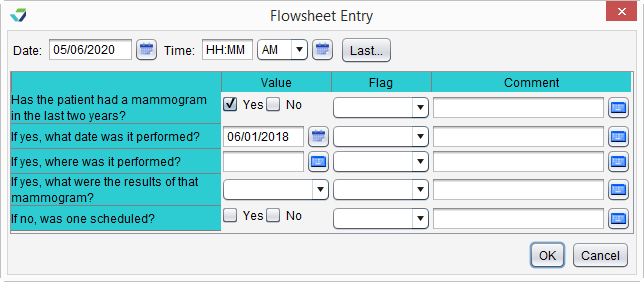
- Go to Encounter > Flowsheets/Labs > Standard Flowsheets
- Click Add New Flowsheet
- Select the Breast Cancer Screening flowsheet and click Add
- Click Add Column
- Select Yes for Has the patient had a mammogram in the last two years?
- Populate a date for If yes, what date was it performed?
- Click OK to save
Return to 2022 eCQMs
Didn't find the answer you were looking for?
Contact Sevocity Support 24/7 at 877‑777‑2298 or support@sevocity.com